
FEMINISING THE FACE
Professor Meningaud - Maxillofacial Surgery at Paris Est Créteil
The ageing of a woman’s face leads not only to skin changes, but also to morphological changes, with facial features losing their femininity.
Treatment can be medical, surgical or a combination of the two, but must be based on a diagnosis and high-quality support, says Professor Jean-Paul MENINGAUD, who details the essential anatomical points on which to intervene in order to effectively (re)-feminise the face.
Feminising the face
Feminisation of the face is increasingly practised in maxillofacial and facial plastic surgery. It concerns gender reassignment, of course, but also a number of syndromes such as acromegaly, the iatrogenic effects of certain hormone treatments, women who feel too masculine without any pathology, and above all the effects of age, which tend to masculinise the face. Surgical or medical techniques are used, and it is often necessary to combine them.
Aetiological diagnosis
We won’t go into detail here, but it is obviously fundamental and can be very complex, particularly in the case of gender dysphoria. In this case, it is a matter for ultra-specialists and can only be made by a well-trained multidisciplinary team, after a negative biological work-up and long-term psychiatric follow-up. Apart from this very special case, a systematic clinical examination should be carried out and, depending on what is found, a number of additional tests should be prescribed. It cannot be stressed enough that medicine and cosmetic surgery are first and foremost medical procedures.
Morphological diagnosis
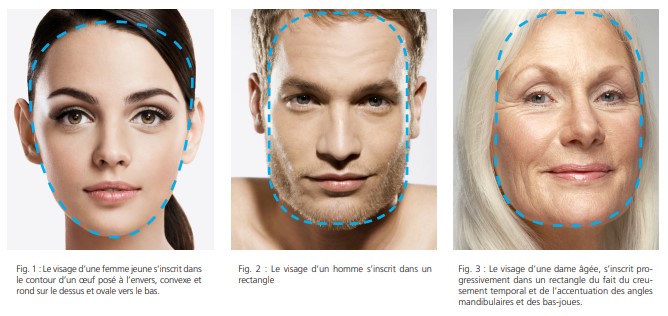
The shape of a young woman’s face is similar to the outline of an egg laid upside down on a table. It is round and convex at the top, and oval at the bottom Fig.1. A man’s face, on the other hand, is shaped like a rectangle Fig.2. It’s no coincidence that many young men trim their beards to give their jaws a more masculine, rectangular shape, particularly if they have a retro-genius or receding chin. As a result of certain syndromes or simply ageing, the contours of a woman’s face tend to become ‘rectangularised’ Fig.3. The temples deepen, the lower cheeks transform the oval into a round and then into a square. The mandibular angles tend to protrude as a result of hypertrophy of the masseters and/or the lower lobe of the parotid glands, and of the mandibular bone. Due to the perspective effect, the zygomatic arches appear less prominent. In profile, the cervico-facial angle is more marked in women than in men. Certain syndromes, or simply age, tend to open up this angle. Finally, wrinkles are generally better accepted in men than in women, probably wrongly so. The morphological diagnosis should be detailed on a diagram, layer by layer. Ideally, photos of the patient’s face and profile should be projected onto a screen and commented on in the form of an open and constructive dialogue. Finally, it may be useful for information and educational purposes to perform a morphing to ensure that the issues have been properly understood. These images are not contractual, and fortunately the result is almost always more convincing than the simulation. For complete feminisation, several consultations are necessary to assimilate the information. When facial feminisation procedures are combined with a facelift, the attractiveness of the face will be significantly improved.
Treatment targets
The upper level
The targets are forehead wrinkles, the temples, the frontal sinus area and the superciliary arches.
Forehead wrinkles
Botulinum toxin should be used sparingly to treat forehead wrinkles, as it can cause eyebrows to droop and ultimately make the eyes appear more masculine. Apart from exceptional cases, bleaching (a difficult but highly effective technique) and/or lipofilling techniques should be used. At Mondor, we use enriched techniques1 and, as a back-up, laser techniques give good results. Our team has scientifically tested a successful Erbium-Yag treatment2.
The temples
If they are hollow, the temples can be treated with volumising hyaluronic acids or lipofilling. The techniques used in reconstructive surgery, in particular cement injections under endoscopic control, are not suitable.
The frontal sinus region
With age, the volume of the frontal sinuses increases, while that of the maxillary sinuses decreases. This leads to protrusion of the glabellar region and the superciliary arches. Treatment is necessarily surgical. In most cases, endoscopically controlled grinding through a punctiform approach is sufficient. In complex cases, a surgical approach is required, with retraction of the anterior wall of the frontal sinus.
The superciliary arches
The position of the eyebrows can be altered at the same time as a temporal lift or using more sophisticated techniques. At Mondor, after using Dr Daniel Marchac’s endoscopic ‘endofront’ facelift technique for a long time, we now use Dr Fausto Viterbo’s technique, which involves direct placement of the eyebrow via a subcutaneous detachment.
The middle layer
The main targets are the nose and the zygomatic arches.
The nose
Everyone agrees that some noses are more feminine than others. Experimental psy- 30 DERMATOLOGY I body language chology studies have shown that a very slightly sunken, thin nose will appear more feminine. With injectables, it is possible to give the impression of a finer tip and erase a slight bump. Otherwise, surgery is required, although it should be borne in mind that the feminisation process involves subtle gestures. With ageing, many patients who had a straight nose at 20 have a hump and a loss of definition at the tip, which tends to masculinise the nose. This is why rhinoplasty to feminise the nose should be considered before any facelift is planned.
The zygomatic arches
Using the egg analogy mentioned above, the zygomatic arches should appear more prominent than the temples or the oval of the face. This appearance can easily be treated with volumising hyaluronic acids or lipofilling. In men, injection of the arch is feminising and should be avoided. In men, only the anterior region known as the valley of tears should be injected. To limit the risks as much as possible, I strongly recommend using cannulas, injecting by backtracking, absolutely avoiding boluses (sources of biofilm and then infection), and routinely using transillumination to avoid bruising. In exceptional cases, orthognathic surgery may be used. Trans-facial profiles (maxilla forward) are more feminising.
The lower level
The targets are the length of the upper lip, the mandibular angles, the chin and the cervico-facial angle.
The upper lip
Feminising the lips is easily achieved by a treatment involving an upper lip lift, a simple technique updated by Dr Cornette de Saint Cyr and performed under local anaesthetic. In addition to the effect on the length of the lip and the uncovering of the upper incisors at the smile, this technique makes it possible to redraw the vermilion, the cupid’s bow and the philtrum. It is most often combined with bleaching (or laser or peeling) techniques for the ‘bar code’ and vermilion injections for volume.
Mandibular angles
The treatment of mandibular angles is spectacular but unfortunately difficult and often surgical. It involves an endo-buccal shaping osteotomy. A mistake often made is to cut the angles, but a woman’s mandibular angles contribute to her attractiveness. They should be feminised but not amputated. In the Middle East, there is a growing demand for so-called ‘Texas’ surgery, which aims to make the mandibular margin, including the angle, more visible. This modelling is often insufficient, and the result is obtained by loosening the masseter muscles. Treatment with botulinum toxin is possible, but very technical and demanding. In exceptional cases, partial surgery of the lower lobe of the parotid gland may be indicated.
The cervico-facial angle
Treatment of the lower lobes is fundamental to treating the oval of the face. Filling in on either side tends to make the face heavier and no longer corresponds to the current philosophy, which aims to fill in the upper regions and free up the lower ones. What remains is the centro-facial lift (at Mondor we perform a trans-osseous attachment) and/or the deep lift.
The chin
The male chin has two paramedian protuberances, whereas the female chin has only one central one. The best technique is transverse genioplasty, which aims to reduce the width of the chin and restore or accentuate the oval. Remodelling of the tuft, which completely disrupts the complex kinetics of the chin muscles, should always be avoided. Depending on the case, this procedure can be isolated or accompanied by an advancement to clarify the cervico-facial angle, a vertical reduction to accentuate feminisation or a recession, but the soft tissues will have to be reorganised to avoid the classic ‘witch’s chin’. Although my technique differs from his, it is Dr Claude Le Louarn to whom I owe the greatest contribution to my understanding of the physiology of facial ageing with his theory of Face Recurve®. For me, the key to a lasting result goes beyond fixing the platysma muscle to a fixed point (the hyoid bone) and lies in releasing the muscle.

The key to success
As always in medicine, the key to success lies in a good diagnosis, high-quality information and support, and perfect mastery of the sequence of planned procedures. The aetiological diagnosis must be unambiguous, and the morphological analysis as accurate as possible. Patient compliance is vital. This requires repeated consultations to allow the decision to mature and the information to be assimilated. This essential time unquestionably contributes to patient satisfaction and the pleasure we derive from practising our profession. Modern teaching tools are important: high-quality photographic documents, morphing, information sheets, commented diagrams, 3D resin models, examples of similar cases, etc. Finally, in my opinion, techniques should be taught in university hospitals, because of the guarantees of independence. At the very least, the procedures should combine medical techniques, and often both medical and surgical techniques.
References
1. Midface rejuvenation surgery combining preperiosteal midcheek lift, lower blepharoplasty with orbital fat preservation and autologous fat grafting. Chatel H, Hersant B, Bosc R, La Padula S, Meningaud JP. J Stomatol Oral Maxillofac Surg. 2017 Oct;118(5):283-288.
2. Multifractional microablative laser combined with spacially modulated ablative (SMA) technology for facial skin rejuvenation. Hersant B, SidAhmed-Mezi M, Chossat A, Meningaud JP. Lasers Surg Med. 2017 Jan;49(1):78-83. doi: 10.1002/lsm.22561. Epub 2016 Jul 18.