

The overlying scalp expands. After a few days, there is enough scalp to close the loss of substance. Despite these techniques, scars can sometimes be quite large and therefore visible. In such cases, follicular micro implantation can be performed. Hair follicles are harvested from the nape of the neck, separated from each other under a binocular magnifying glass and re-implanted one by one.

Patient presenting with a large alopecic area as an after-effect. Expansion prostheses were placed on both sides. They were progressively inflated with saline. When the prostheses are removed, the resulting scalp will enable the alopecia area to be removed and the loss of substance to be closed up without difficulty.
How are lips repaired after cancer?
The lip is not only a very important aesthetic component of the face, it also performs fundamental functions. It is involved in phonation and the retention of saliva and the alimentary bolus.
This function is performed by muscles, one of which is essential: the orbicularis muscle. Reconstruction of the lip must therefore take this muscle into account.
Repair of full-thickness loss of substance of the lip aims to reconstruct the mucosa, the muscular webbing and the skin. When direct closure is not possible, the main repair method is to use the opposite lip. This is tilted either in a single or two-stage operation.
How is the oral cavity rehabilitated after cancer?
The removal of certain tumours from the oral cavity can make it difficult to fit dental prostheses, for a variety of reasons: bridges, insufficient bone, difficulty in opening the mouth, communication between the mouth and the nose or sinuses. For each after-effect, a restorative procedure can be proposed: bone grafting, maxillofacial prosthesis, flange plasty, action on tendon insertions, bone correction, etc.
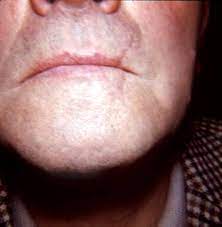
How are lips repaired after cancer?

Cancerous lesion of the lower lip

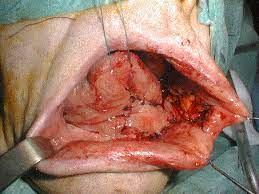
How is the oral cavity rehabilitated after cancer?

Patient with cancer of the floor of the mouth. Absence of vestibule prevents correct placement of an adjunctive prosthesis. Harvesting of a buccinator muscle flap from the inner surface of the cheek to reconstruct the anterior floor.

Does surgical repair of facial cancer comply with ethical rules?
Any surgical procedure requires an assessment of its benefits and risks. An operation is only acceptable if the benefit outweighs the risk. Often, several techniques can be used to obtain roughly the same result.
The surgeon takes the risk-benefit ratio into account when proposing one technique rather than another. What’s more, the repair procedure must not be to the detriment of cancer surveillance possibilities.
Lastly, the choice of a restorative procedure is made in such a way as not to make a second procedure impossible. The surgeon takes into account the possible failure of the first procedure. These are some of the ethical rules that guide cancer repair.
What is epithesis repair?
Epitheses are plastic prostheses used to simulate a nose, ear or part of the face. Two major advances have considerably improved the quality of this type of reconstruction. The first is the use of silicones for these prostheses. It is now possible to obtain very natural appearances in terms of both colour and texture.
Secondly, it is now possible to clip these prosthesis onto implants fixed in the bone. Previously, prostheses were attached to glasses, for example, in such a way that the seam with the patient’s skin was noticeable. This type of reconstruction is often dismissed as artificial. This is wrong for two reasons.
On the one hand, in some cases, surgery will only allow a very imperfect reconstruction, whereas epithesis will certainly be artificial but will give an extremely natural appearance. Secondly, epithesis offers an enormous advantage in terms of monitoring local recurrence.
All you need to do is remove it to monitor the surgical site. The possibilities of implant-fixed epitheses are sometimes limited by the lack of bone; this is often the case for the nose and orbit. Advances in bone grafting have considerably increased the chances of success for this type of repair.
How is facial paralysis repaired after cancer?
When the surgeon is obliged to cut the facial nerve because of a tumour, immediate repair by nerve grafting is neither always possible nor recommended. As a result, many patients suffer from the after-effects of facial paralysis. Conventional techniques did allow the face on the paralyzed side to be re-tensioned, but in a static manner. In other words, it was not possible to restore the dynamics of the smile. It is now possible to move the tendon of a muscle (the temporalis muscle) and fix it at the corner of the mouth.
When this muscle contracts, it attracts the corner of the mouth to itself. Re-education then enables the muscle to contract involuntarily, as in a spontaneous smile.
How is jaw cancer repaired
Cancers affecting the facial bones, and in particular the jaws (mandible, maxilla), have benefited from microsurgery. When a large part of the mandible has to be replaced, conventional techniques are not entirely satisfactory. Microsurgery makes it possible to remove a large fragment of bone from the patient and transplant it to the face. This bone can be taken from the leg (fibula) or the hip (iliac crest), for example.
The bone is removed in such a way that the patient can continue to walk as before. The bone fragment is accompanied by an artery and a vein to ensure its blood supply and vitality. Microsurgery makes it possible to perform a bypass operation using a neck artery and vein. When the loss of substance simultaneously involves the soft tissues of the mouth and face, it is possible to reconstruct them at the same time.
The bone fragment can be removed using a skin paddle. These procedures are time-consuming, especially when reconstruction is performed immediately after removal of the cancer. The risk of failure is estimated at 10%. An overnight stay in intensive care is the norm. The average hospital stay is two weeks.
The patient may benefit from radiotherapy if this proves necessary to treat the tumour. Next comes the problem of prosthetic rehabilitation (dentures).
While this was virtually impossible with conventional techniques, microsurgery has made it possible. The result has been further improved by prostheses stabilised by dental implants.
Dental implants can be fixed in the reconstructed bone. If the bone is not thick enough, it can be gradually thickened using a device known as a distractor.
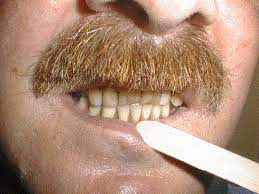
Result after placement of a denture

How is skin cancer repaired?
These cancers have increased dramatically due to the fashion for tanning. Surgical excision most often results in a definitive cure. The difficulty lies in the repair procedure. Tumours located around orifices (eyelids, lips, nostrils) can cause significant after-effects. The techniques used consist of skin grafts or local flaps.
Skin grafts can be taken from behind the ear, for example. It is placed over the loss of substance using stitches. A compression bandage keeps it firmly in place. The graft usually takes five days to set. Local flaps are skin fragments placed next to the loss of substance.
They are designed to respect the aesthetic lines of the face. Ideally, the scars are eventually blended into the fine lines of the face. Skin flaps are moved by sliding, rotation or transposition. These procedures are generally performed under potentized local anaesthesia. This type of anaesthesia minimises risks.
The patient is not completely asleep. The patient is not placed on artificial ventilation during the procedure. However, an anaesthesia consultation is mandatory prior to the procedure.
An anaesthetist is present at the patient’s side throughout the surgical procedure. As a rule, these procedures last less than an hour. They are increasingly performed on an outpatient basis, meaning that the patient goes home on the evening of the operation.


Immediate result of local flap reconstruction

Result one month after surgery.