
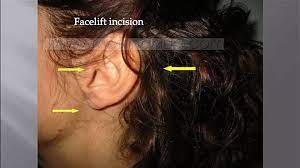
Is the facelift scar dangerous for the facial nerve?
No. In fact, it offers a very wide and imperceptible approach. Cervical approaches should no longer be used.

Who should I contact for a parotidectomy?
Maxillo-facial and cervico-facial surgeons are the surgeons most accustomed to performing this procedure. The key is to use an experienced surgeon.
What is the expected hospital stay following a parotidectomy?
In the past, it was always two to four days. In fact, it essentially depended on the drainage. Now, in many cases, it is possible to use a technique that reduces the risk of haematoma to zero, so that the operation can be performed on an outpatient basis.
What is acute parotitis?
There are three types of acute parotitis
Acute bacterial
Acute parotitis is most often found in weakened patients, such as the immunocompromised, the elderly, diabetics, cachexia, dehydration and salivary lithiasis.
The clinical picture associates a clear infectious syndrome with fever and altered general condition, and a highly inflammatory, tense parotid swelling with pus discharge into the mouth.
Hospitalisation is often required. Treatment is based on intravenous antibiotic therapy or, in the case of abscesses, surgical drainage.
Viral
Most often bilateral.
* Mumps: uni- then bilateral, notion of contagion, sensitive swellings with inflamed Stenon (saliva evacuation orifice in the mouth) and moderate infectious syndrome.
Other viruses :
* Coxsackie A (herpangina), HIV, CMV, influenza, NMI

The illustrations are not photographs, but sketches made by the author, highlighting with dotted lines the targeted areas (face and neck) for rejuvenation surgery. Results may vary from patient to patient, depending on skin condition, lifestyle, age and general state of health.
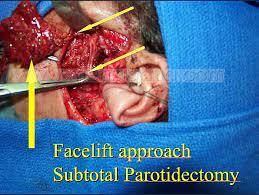
When a pleomorphic adenoma is suspected, is total parotidectomy necessarily required?
This tumour is often finely encapsulated (capsular effractions are frequent in the form of pseudopods or satellite nodules), so any dissection in contact with the tumour should be avoided. Dissection in contact with the tumour (enucleation) carries a high risk of recurrence (20-45%). In addition, the risk of facial paralysis is increased in the event of re-operation.
Multicentric localizations of pleomorphic adenomas (two or more tumour nodules) are exceptional, but do occur. On the other hand, an excessive safety margin of healthy glandular tissue, as in total parotidectomy, does not seem justified either. For this reason, a subtotal parotidectomy may be indicated. This is not an issue for tumours of the deep lobe or those in close contact with the dividing branches of the facial nerve. In the case of isolated superficial lobe tumours, where intraoperative findings ensure that there has been no capsular exposure, partial superficial parotidectomy may be discussed. The advantage of isolated superficial parotidectomy, especially if it is partial, is that it reduces the incidence of paresis. However, it must not be carried out at the cost of incomplete tumour removal.
Does parotidectomy require dissection of the facial nerve?
Not dissecting the facial nerve means running the risk of cutting it. The nerve must be located starting from its trunk, then following its branches, or retrograde in simple cases, which fortunately are the most numerous. Above, a dissection of the facial nerve in a complex case.
What are the most common post-operative risks and sequelae?
- facial paresis
- Frey’s syndrome
- visible scarring
- skin depression in the operated area.
There are techniques that can greatly reduce these risks. For example, facelift scars are often imperceptible. The SMAS flap reduces the incidence of Frey syndrome from 30% to 4%. What’s more, it can easily be treated by botulinum toxin (Botox) injection. Skin depression is no longer visible after the SMAS flap. When partial parotidectomies are indicated, there is often no post-operative paresis. If paresis does occur, it lasts only a few weeks, unless total dissection is necessary, but this is rare. Finally, if sectioning of the facial nerve is necessary, which is exceptional, microsurgery with possible grafting is performed immediately.
What is the clinical presentation of a pleomorphic parotid adenoma?
Classically, it’s a woman who consults for an isolated parotid nodule of recent onset; but this tumour can also concern men.
Clinical examination :
Single, rounded, painless, firm mass, more or less mobile in relation to the deep plane, normal skin opposite with no associated symptoms (in favour of benignity):
* No sensitive (V) or motor (VII) involvement of the face,
* No adenopathy, no spontaneous or provoked pain,
* No alteration in general condition.
The specialist will specify the firmness of the lesion, its size, which may vary between two examinations, characterising its evolution by flare-ups, and will note these elements on a dated diagram.
His clinical examination will look for a malignant lesion of the face (rule out a metastatic lymph node): scalp, nose, orbit, ear. Finally, the other salivary glands are examined (normal in this case).

Example of a patient presenting with a mass projecting into the parotid area and referred to the specialist on suspicion of pleomorphic adenoma. The specialist’s clinical examination will easily re-establish the diagnosis. In fact, it’s a simple sebaceous cyst (adhering to the skin) which can be removed under local anaesthetic on an outpatient basis (15-minute procedure, no parotidectomy).
What does facial paresis look like?

In cases of total parotidectomy, facial paresis is frequent but not systematic. It depends on :
– tumour location: the farther a tumour is located from the trunk, i.e. close to the mouth or eye, the more frequent it is, but the more limited its extension.
– the patient’s age: a young patient is less likely to develop paresis, and if not, will recover more quickly
– the surgeon’s gestural experience: “the flight hours of an airplane pilot are the operating hours of a surgeon”.
– the fact that this is a first operation and not a repeat operation, since a second operation considerably increases the technical difficulties and therefore the risks. For this reason, this is an operation that must be carried out as thoroughly as possible, so that the first operation is also the last.
Facial paresis is incomplete facial paralysis. It is linked to the interruption of the small vessels that irrigate the nerve (the vasa nervorum). Performing a SMAS flap accelerates nerve recovery. This faster recovery is thought to be due to the vascular richness of the SMAS.
Numerous tests are available to measure its intensity. These tests enable specialised physiotherapists to guide functional rehabilitation.
Of course, facial paresis is most noticeable in facial expressions. That’s why a photo doesn’t really show what paresis looks like. To simplify matters, there are two main areas affected: the eyes and the mouth:
– As regards the eyes, from the least to the most severe: asymmetry of blinking, slowed closure of the upper eyelid, exceptionally absence of eyelid closure, with risk of corneal ulceration.
– Concerning the lips, from the least severe to the most severe: slight asymmetry of the lips noticed by the professional and not by the patient, frank asymmetry in mimicry noticed by the patient, exceptionally significant asymmetry causing speech difficulties.
Facial paresis is transient, with recovery the rule. It must be distinguished from facial paralysis (complete paralysis over a sector): this is linked to the accidental or voluntary (cancer) severing of a nerve branch.
Some surgeons organise patient chains. Each patient to be operated on is received by the last to be operated on. He in turn receives the next patient. At best, the chain is split into female and male members, as the concerns of each are not always superimposable.
Can the facial nerve take an unusual form?

Example of a highly anastomotic facial nerve: Tortella plexus type
I'm going to have a parotidectomy, will i be short of saliva?
Rest assured, you won’t run out of saliva, as you’ll retain your second parotid gland, your two submandibular glands, your two sublingual glands and an infinite number of accessory salivary glands. Problems with salivary secretion occur mainly in patients who have undergone radiotherapy, or in patients with diseases affecting all the salivary glands, such as Gougerot Sjögren’s syndrome.
What is a pleomorphic adenoma?
Pleomorphic adenomas, or formerly mixed tumours (epithelial-myoepithelial component and conjunctival or stromal component) of the parotid gland, are benign, slow-growing tumours. They are common (60% of parotid tumours) and affect middle-aged adults (in their forties), with a female predominance (around 3/1). These epithelial and mesenchymal tumours are poorly encapsulated (invasion of the capsule by pseudopods and satellite nodules), which contraindicates enucleation (recurrence). Exceptionally, they may be multifocal (2 different nodules).
What does a pleomorphic adenoma look like on a ct scan?
In this case, it was a recurrence of a pleomorphic adenoma. The patient had not undergone a subtotal parotidectomy, but a simple enucleation. Today, MRI is the preferred option.
What is frey syndrome?
Hypersudation and erythema (redness) of the temporal region during meals due to erroneous reinnervation of the sweat glands by the auriculo-temporal nerve (treated by botulinum toxin injection, incidence reduced by interposition of a SMAS flap).
Preventive treatment
The SMAS flap visible in the photo (superficial musculoaponeurotic system) fills in the loss of substance and attenuates retro-mandibular retractions. It reduces the incidence of Frey’s syndrome by interposing itself between the two nerve contingents (incidence down from 33% to 4%). The few Frey syndromes that occur with this technique seem to be due to SMAS flaps that are too thin or perforated during dissection and not repaired. This flap also appears to improve nerve recovery (from 3 months to six weeks). Some teams interpose different types of implants (acellular dermal matrix, for example) with encouraging results.
Curative treatment
Since 1994, the curative treatment of choice has been botulinum toxin A. A Minor’s test is sometimes necessary to better identify the areas to be treated. The skin is prepared with an anaesthetic ointment. Injections must be intracutaneous to avoid causing facial paralysis. Results are excellent, with a negative Minor’s test after one week. Re-injections are sometimes necessary, but the results are still very good.
The MINOR test: the skin of the parotid region is coated with an iodine solution and then dried. The area is then sprinkled with starch. The patient is then given a vitamin C tablet or a piece of lemon to chew on. Hypersudation then turns the areas affected by the syndrome blue.
How much does a parotidectomy procedure cost?
In France, 100% of the cost of parotidectomy is covered by social security.
However, practitioners working in sector 2 of the French health system may charge higher fees. Mutual insurance companies may cover all or part of these extra fees. The rate of reimbursement depends on the contract taken out. The easiest thing to do is to ask for an estimate of the procedure, including the amount of the extra charge, and to check with your mutual insurance company.
Who are the practitioners authorised to set up in sector 2? The sine qua non condition is to have been a chef de clinique or hospital assistant for at least two years.
Is it possible to perform a partial parotidectomy under local anaesthetic?
Yes, in some cases it is possible. A light sedation is generally associated. This is known as potentiated local anaesthesia.
What are the risks of tumour enucleation without parotidectomy?
Enucleation consists in removing the tumour, leaving most of the gland behind, usually by direct approach to the nodule. This procedure is not recommended, as it presents a number of risks:
Some tumours, such as CALP, tend to be multi-focal (i.e. have several locations within the gland). Simply removing the main mass can lead to the proliferation of other lesions. Any further surgery increases the risk of facial nerve damage.
Some tumours (pleomorphic adenomas) are poorly encapsulated (capsule dehiscence with pseudopods and satellite nodules), also running the risk of recurrence.
Enucleation using a direct approach to the nodule, i.e. without locating the facial nerve branches, runs the risk of severing a branch.
Finally, parotid tissue left in place increases the risk of salivary fistula (leakage of saliva through the scar).
Can you explain the anatomy of the parotid gland?
The parotid gland is connected to important vascular and neural elements:
The facial nerve (VII) divides into two branches (temporofacial and cervicofacial) between the superficial and deep lobes of the gland, then branches into a fine network that becomes increasingly superficial. (DANGER during surgery)
The external carotid artery gives rise to two terminal branches in the parotid lodge on the inside of the gland: the superficial temporal artery and the internal maxillary artery.
The external jugular vein crosses the facial nerve between the two lobes of the parotid gland.
The auriculotemporal nerve penetrates the upper pole of the gland, stimulating salivary secretion.
Numerous lymphatics border the gland and vessels.
Is a ct scan useful in the assessment of a parotid tumour?
When the clinical examination of a parotid mass is negative (absence of facial paralysis), a CT scan is of little use. The diagnosis is made by removal of the gland and histological analysis.
On the other hand, when the clinical examination suggests a malignant tumour or a very large tumour, a CT scan may be useful in guiding the surgical procedure.
A CT scan is not used to decide whether or not to operate (i.e. to establish the indication), but may be used (in a few rare, very specific cases) to guide the surgeon during the operation.
Today, it is much better to perform an MRI, which will be much more helpful in determining the benign-malignant diagnosis.


Parotid calculi (lithiasis) : diagnosis? treatment?
PAROTID CALCULI
INTRODUCTION
Parotid lithiasis is much less frequent than submandibular lithiasis, as saliva is poorer in mineral salts and more fluid in the parotid gland. They are usually asymptomatic and are discovered by chance.
CLINICAL HISTORY
The clinical symptomatology is the same (salivary hernia or colic), punctuated by meals and in the form of swelling of the pretragal or retro-mandibular region.
Infectious accidents are possible (stemonitis, parotitis, pericanal abscess), but lithiasis is more difficult to diagnose, as the stones are often numerous, small and radiolucent in 20% of cases.
RADIO
Endobuccal (genian portion of the Stenon) and extra-oral X-rays look for radiopaque calculi.
Hirtz incidence
In this case, sialography has a broader indication, enabling small or radiolucent calculi to be identified.
TREATMENT
Initially mainly medical (antibiotics, antispasmodics, etc.).
Surgical :
increasingly, endoscopic excision
Exceptionally, superficial parotidectomy for distal or glandular calculi;
Lithotripsy is indicated provided the gland is functional.
Sarcoidosis or besnier-boeck and schaumann (bbs) disease and the parotid gland, diagnosis? treatment?
BBS disease gives rise to two syndromes:
Mikulicz syndrome: bilateral, painless, chronic swelling of the parotid and other salivary glands, as well as the lacrimal glands, sometimes with reduced or suppressed secretion.
Heerfordt syndrome: usually febrile condition combining bilateral parotid and lacrimal gland hypertrophy (reminiscent of Mikulicz syndrome), bilateral uveitis and peripheral facial paralysis (differential diagnosis: malignant tumour), more rarely III and VI paralysis, mild meningeal reaction. This uveo-parotitis is classified as BBS disease.
Diagnosis is made by biopsy and histological analysis. Treatment is that of BBS disease, essentially with corticosteroids.
What is the advantage of the retrograde approach for the facial nerve?
When it is possible (the tumour must be inferiorly polar, but this is frequent), it is quicker and reduces the risk of facial paresis. The postoperative period is much shorter.
Is drainage essential?
No, there is a new technique that avoids drainage while guaranteeing the absence of hematoma.
Is a neurostimulator essential for locating the facial nerve?
No, it can even be a false security. You should have one, but only use it in very special cases.
What about cytopuncture and biopsy?
Cytopuncture, provided it is interpreted by an experienced cytologist, can in many cases lead to a diagnosis. There is, however, a risk of pricking next to what we want to analyse (a focus of carcinogenesis within a tumour). Ten percent of examinations are non-contributory due to insufficient cells in the sample. The risk of swarming by fine-needle puncture (25-gauge) seems theoretical if the sampling technique is correctly performed. Three punctures per tumour are nevertheless necessary to limit the number of non-contributory cytopunctures. The reliability of the malignant or benign diagnosis is not absolute (around 92%). Discrimination between the different types of benign tumours (83%) and malignant tumors (less than 50%) is more difficult. Combining this examination with MRI improves efficiency, without however achieving 100% efficiency.
Histological examination of the entire gland is by far the most reliable.
Biopsy is contraindicated, as there is a high risk of facial nerve damage and the spread of cancer or pleomorphic adenoma.
